The following account of the route of evacuation of the wounded soldier on the Western Front from the trenches to the Base Hospital or to England is taken from a series of essays, published by the British Medical Association in 1917, and is reproduced here by kind permission of the the British Medical Association.
The route of evacuation is described in detail and include stretcher bearers, Battalion Medical Officers, Regimental Aid Posts, Advanced Dressing Stations and Field Ambulances, Casualty Clearing Stations, the operating theatre trailer, ambulance trains and barges and evacuation back to England by Hospital Ship.
Reference should be made here to the war drawings of Muirhead Bone that illustrate the evacuation by barge and hospital ship. Muirhead Bone's drawings will be found at: http://www.ku.edu/carrie/specoll/medical/mbone/mbonedex.htm
Dr M G Miller, Editor
THE ROYAL ARMY MEDICAL CORPS AND ITS WORK
THE general work of the medical service of the British army may he regarded as falling into three main sections:
1. The physical and environmental hygiene of the soldier's life.
2. The evacuation of sick and wounded from places at which their presence is an obstacle to the success of military operations, and detrimental to the man themselves; and
3. The provision and maintenance of institutions at which sick or wounded soldiers can remain during treatment.
In theory, and to some extent in practice, the area in which the work has to be done is divided into three zones. The first or forward area is known as the "collecting zone" (Fig. 1).
Fig. I.
Collecting Zone. Diagram representing the distribution of the medical units. The plain circles are regimental aid posts. The circles with a dot in the contra are advanced dressing stations, and those with a cross are main dressing stations of field ambulances. The circles with a vertical line through them are rest camps and other annexes to main dressing stations. The upper oblongs are a couple of casualty clearing stations connected by road with the field ambulances and with the base by a railway line and canal traversing the evacuating zone. The oblong below (S.H.) is a stationary hospital in the evacuating zone. Opposite it is an advanced depot of medical stores (A.D.).
In it the wounded are collected from the battle-field, and the sick from the places at which they fall ill.
Theoretically it is an area of the shape of a triangle, connected by its apex with the lines of communication, and having at its base the regiments in action; and nominally it contains only the regimental aid-posts, the field ambulances, and a "casualty clearing station," or railhead hospital, which stands at the apex, and serves to house the sick and wounded sent on from the field ambulances until they can be passed down through the evacuating zone to the distributing zone. In practice, however, it contains certain other units of a medical character.
The next or middle area is known as the, "evacuating zone," because it is traversed by the roads, railway lines, or canals along which the sick and wounded are carried on their way to the distributing zone. It corresponds with the military area known as the lines of communication, and, theoretically, is long and narrow, containing, from a medical point of view, nothing but the various means of transport, and perhaps a medical store or two and a few "stationary" hospitals for the reception of patients who should not be taken any further towards the distributing zone.
The third or lowest area is called the "distributing zone," because in it are placed the various institutions among which the sick and wounded are to be distributed to receive their final treatment. It is an area of indefinite size, corresponding roughly to that in which munitions of war are gathered and reinforcements collected, and which, from a purely military point of view, is known as the base. In this war it lies partly in Great Britain, partly overseas, and consequently it is common to speak of it as if it contained institutions of two different orders - "home hospitals" and "overseas or base hospitals."
The collecting zones in France may be regarded as divided into sections, each with its own line of communications and a railhead, for the front is actually held by different armies each of which has its own area of operations. Each such area is in medical charge of a senior medical officer known as Director of Medical Services (D.M.S.), who is responsible for the arrangements he makes only to the general of the army to which he belongs, and to the principal medical officer of the British forces - that is to say, the Director-General of Medical Services on the staff of the Commander-in-Chief.
In the collecting zone, even in parts of the area full of suggestions of the industries of peace, the dull booming of the guns is rarely inaudible, while a few miles further afield the road is encumbered from time to time by ammunition waggons, by ambulances, by fresh battalions going up to take their place in the line, or by battalions returning to their billets mudstained and worn. The hill tops, too, disclose a view perhaps of swiftly moving aeroplanes, a line of observation balloons, and the rising smoke clouds formed by bursting shells. This area has an atmosphere all its own - bracing, suggestive, thrilling, yet curiously solvent of illusions and of personal petty ambitions. That is its effect, at any rate, on many a newcomer. He sees himself suddenly from a new angle; he recognizes that he has arrived at a place where there is no room for the looker-on at life, at a place where men justify their existence by work and their deaths by altruistic aims, and where nothing counts but the war.
The various sections of this zone are each, as has been said, in charge of a director of medical services, who works through the deputy directors (D.D.M.S.) in charge of the corps into which every army is divided, and these again through the assistant directors (A.D.M.S.), who are responsible for the medical work of the divisions out of which army corps are constituted.
The number of men in a division is roughly 20,000, and to meet their needs each A.D.M.S. has at his disposition the personnel of three field ambulances, and twelve or more medical officers attached to single battalions or like divisional units.
BATTALION MEDICAL OFFICERS.
The battalion or regimental medical officers do their work in a more advanced position than any others, and in some respects are the most important components of the whole medical service.
Each is as it were the family medical attendant of the men of the unit, the medical officer of health of the locality in which it may for the moment find itself, and the private medical adviser of the commanding officer - in respect of all questions in which medical considerations arise. He gets, or should get, to know the mental and physical peculiarities of every officer and man in his battalion - knowing, for instance, such things as who have dubious feet, who a nervous constitution, who are exceptionally hardy, who are careless in their living, who careful, who are disposed to go sick on the least excuse, who will never report themselves until positively obliged. He acquires this knowledge by going about among the men, by his formal medical inspections and by noting who are the frequent attendants at his morning sick parades, and why they come. Bearing in mind that the sole reason why the men are in his charge at all is in order that they may fight, and fight effectively, he treats them much in the spirit of the medical attendant of a racing crew. Hence he is always endeavouring to tackle small evils early, and to winnow out the sick to whom he can afford all necessary treatment himself from those who must be sent elsewhere.
Everything that can in any way affect the health of his unit comes within his purview: food and its preparation, the sterilization of the water supplies, the provision of latrines and their proper maintenance, the destruction of rubbish, and the cleanliness of billets and dugouts. He is always, too, on the alert for the first signs of an outbreak of any epidemic malady, wages war on parasites and flies, and endeavours to ensure that the men appreciate the importance of the various precautions they are told to observe, including those against trench feet. His authority he derives partly from his personal position, partly from his influence with the commanding officer of his battalion. if he secures the confidence of the latter, and the real respect of the adjutant and the sergeant-major, his work is, from one point of view, easy.
His duties are continuous, whether his unit be resting in billets or be taking its turn in the fighting line.
TRENCH WORK.
If it be taking its turn in the fighting line he has also to attend to battle casualties and their evacuation, his precise duties in this connexion differing according as trench fighting is in progress or an "over the top" advance.
In the former case he does his work from a predetermined point chosen according to the lie of the ground and other circumstances, at or close sometimes to the head quarters of one of the companies of the battalion or sometimes to those of the battalion itself. The former are likely to be in a dug-out or trench some two or three hundred yards behind the fire trench, and the latter perhaps twice or three times that distance (Fig. 2).

Map, drawn from memory. Showing the position of a certain regimental aid post lying between a main and an accessory communication trench. The shaded block is the post itself. It stands across the trench, the patients approaching along the curved trench and leaving by the straight descending trench, which leads to the advanced dressing station. The ascending arm leads to and from the firing line. The projection (L) is the latrine. The small shaded projection (S) is a dugout for four RAMC stretcher bearers.
Here he establishes a first or regimental aid post, equipping it with the ordinary provisions of a surgery, coupled with bunks or other lying-down accommodation for, say, half a dozen seriously wounded men (Figs 3 and 4).
Fig. 3 - Ground plan of a regimental aid post shown in elevation in Fig. 4. On the left (O) is a bunk for two orderlies, each having his stretcher bed; next is the MO's bunk, with a stretcher bed and table. In the centre compartment running from entrance to exit are trestles to support a stretcher while a case is being dressed, some tables and shelves for bottles and instruments, and two sitting benches. On the right is an empty space for storing the kits of patients, and beyond are slides, each to hold three stretcher patients in tiers. curtain separates them from the centre compartment. Gas-proof curtains are rolled up above the doors ready to let down on a gas alarm, and on the floor near the exit is a cylinder of oxygen and spraying machine and some bottles of anti-gas solution.
Fig. 4.
Elevation of the regimental aid post shown In Fig. 3. Tiers (S.P) for stretchers for patients
are seen on the left (one in position) and the M.O.'s bunk and stretcher bed on the right.
In the middle is a trestle to support a stretcher while the case is being dressed and near it a bench for bottles
and dressings. Sufficient height for work (about 6 ft. 6 in.) is secured by slightly deepening the trench, inflow
of water being prevented by a dam and sump pit. The floor is concrete, the roof, concrete, sand. bags and earth.
Light is supplied by acetylene lamps.
The aid post itself may be the cellar of a ruined cottage or house, a deserted German dug-out, or an ostensibly shellproof annexe to a communication trench, but whatever its nature he endeavours to guard his patients against a gas attack, providing for all openings a blanket screen soaked in an anti-gas solution wich can be lowered into place at a moment's notice. Also, if the accommodation of the post be at all considerable, he takes what steps he can to divide it up in such fashion that no single shell is likely to affect all parts of it.
To assist him he has a corporal and four men of his own corps, their specific duty being to look after the water supplies he draws from the battalion a lance-corporal, a driver for the small cart in which he carries about his aid-post outfit, and from each half-company one man whose specific duty is sanitation. The unit, also supplies him with men to act as stretcher-bearers in the proportion of two to each half-company, or sixteen in all. His total command therefore consists of twenty-nine men, all of whom he trains in stretcher-bearer and first-aid work, but otherwise employs as he finds advisable. Subject to the specific duties mentioned he usually posts most of his men along the trenches held by his unit in order that they may be ready to attend the casualties when the cry "stretcher-bearer at the double" is passed from sentry to sentry. The medical officer visits the fire trenches whenever occasion occurs, and often merely to encourage the men by the knowledge that should they be wounded skilled attention is at hand; his assistants are, however, competent in ordinary cases to apply the first aid dressing which every soldier carries inside his tunic; if feasible, the wounded man is then removed to the regimental aid post. Consequently, it is here that the medical officer habitually, remains.
If, however, the injury be a fracture of the lower limb or other serious condition, or the man cannot be brought back to the aid post forthwith, the medical officer goes up to see that the necessary steps are taken. These will always include the placing of the patient in some position in which be will be out of the way of the fighting men, while if the trench be waterlogged or the weather very rainy, and the patient helpless, it may be, necessary to build him up a bed out of a stretcher on the fire-stop (Fig. 5), or elsewhere above the water line, protecting him from cold and wet by blankets and a water- proof ground sheet.
Fig. 5.
Diagram representing a section through a fire trench, measuring about 2 ft. at the bottom, about 4 ft. at the upper ground level. and about 6 ft. 6 in. from top to bottom. The shelf at the side, or fire-step, can be used as the foundation for a stretcher bed when the bottom of the trench is full of water.
The difficulty of getting a case out of the trenches varies with its nature, with the amount of the fighting that is in progress, and with the character of the trench leading from the place where the casualty has occurred to battalion head quarters. A plan of a common type of trench is shown in Fig. 6.
Fig. 6.
Outline of a common form of trench with traverses projecting towards the rear. The straight parts are the fire bay; on the left is the beginning of a communication trench. On the right is a latrine (L) leading out of a traverse. Many of the angles of such a trench are worn away.
Should the communication trench have been knocked about recently or be waterlogged, it may not be easy even for an active and unloaded man to go along it, and in the best of circumstances the transport of a wounded man along the trenches is a problem presenting much difficulty.
Certain types of new trench (Fig. 7)
Fig. 7. - Diagram of a type of trench presenting special difficulties in moving wounded men It is a twin trench of which the front one is never more than about 2 ft. wide and 4 ft. 6 in. deep.
may be nowhere wider than 24 in., while the average width of a fully- developed trench is not more than 4 ft. at the level of the shoulders, and its course is invariably interrupted by angles round which an ordinary stretcher cannot be carried except by tilting. (Figs. 8 and 9.)
Fig. 8 -Diagram to illustrate the difficulty of getting a stretcher round the angles of
a trench.
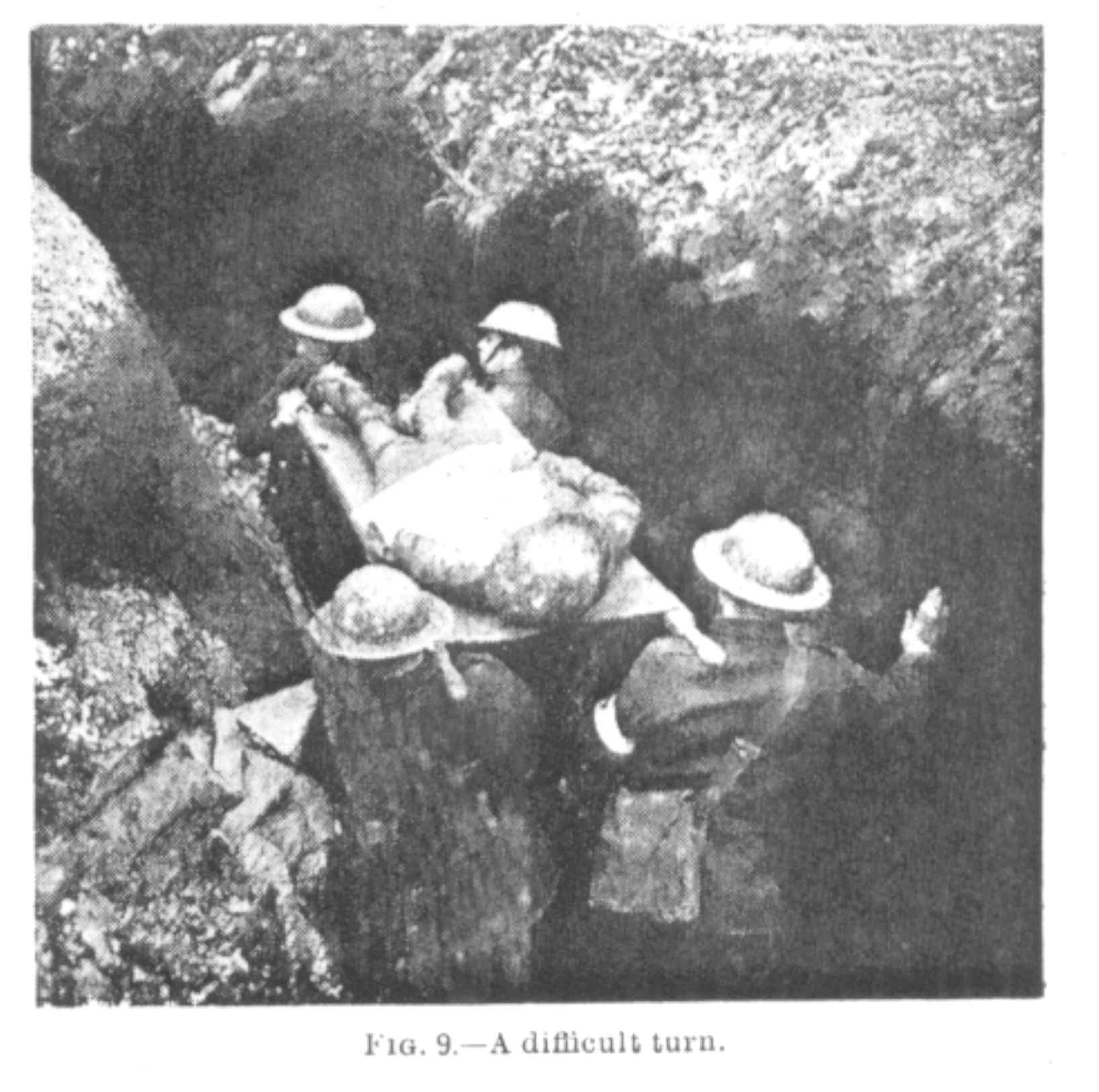
Numerous special stretchers have been devised, and some of them meet their purpose if the communication trench is good, and especially if the trench in which they are being used, be an old one and the corners of the traverses worn away.
Fig. 10 is a diagrammatic section of another type of trench in use where the ground water level is sufficiently low to allow a depth to be given to the trench sufficient to protect from rifle fire a man a little over six feet high.
Fig. 10
There are, however, many cases, as also many trenches, in which the special stretchers are unusable, so it is common for the problem to be solved by lifting the patient on a blanket or on a stretcher over the parados or back wall of the trench, and carrying him to the regimental aid post over the intervening ground. Should the trench happen to lie at the top of an ascent this is a relatively easy process, but otherwise it can only be carried out after nightfall unless the need for removal is so urgent that the risk must he taken of the patient and his bearers all being killed.
When the patient arrives at the aid post every care is taken to obviate shock as far as possible by the administration of morphine and hot drinks, and by protection from cold. A label is attached to the wounded man briefly describing the nature of his injury, and, if some time is likely to elapse before he can be removed out of the firing line altogether, a dose of tetanus antitoxin is given. The medical officer's outfit includes everything necessary for such purposes, as also for the arrest of haemorrhage, the splinting of fractures, and the antiseptic treatment of wounds; but he is not expected or desired to undertake formal operations.
WORK IN THE OPEN.
If the unit to which he is attached be taking part in an advance, the duty of a battalion medical officer usually requires him to wait till the attack has been launched. As soon as he sees reason to believe that his battalion is holding its own, but that casualties are occurring, he advances with his men and hunts for a spot where he can establish a regimental aid post.
If the area over which the attack is to be launched is well known because previously occupied or successfully reconnoitred by aeroplane or other observation, the front- line maps prepared for the use of the head quarters of the battalion going into action or occupying the front trenches may indicate to the medical officer where he is likely to find a good place for his regimental aid post. Otherwise he must trust to his own judgement and enterprise, selecting a dip in the ground, an enemy trench, a mine crater, a large shell hole, anything that will serve to protect his wounded from direct fire; in any case it is, if possible, near a road. He starts as soon as possible, not only because his services are needed, but also because the enemy, as soon as the attack has been launched, is likely to try and cut off the arrival of supporting troops by a curtain of shell fire.
His regimental aid post having been established, and any patients that had been brought to it having been duly treated, the NCO probably goes to see cases which his orderlies have found, but have not been able to move, or to which his attention is otherwise attracted. For these he does what he can, and if they cannot be moved to the regimental aid post on account of their condition or the heaviness of the fighting, he tries to collect them into groups, so that they can be found again easily and moved later on. If the area over which his battalion has been fighting is extensive, he perhaps leaves an orderly in charge of the larger groups. The whole of this work is highly dangerous, since, apart from being done under rifle fire, the artillery fire intended to prevent the arrival of supporting troops often affects the neighbourhood in which the M.O. and his men are necessarily working.
Of the men who are not so seriously wounded as to be unable to walk, a good many probably find their way straight to the rear after applying their own field dressings or getting them applied by a comrade. Others make their way to the regimental aid post, and there they remain with the stretcher cases until their wounds have been dressed and the firing slackens sufficiently to enable them to make their way to the rear.
The stretcher cases remain until ambulances come up to fetch them, and unless the fighting is very heavy this process of evacuation will begin very shortly after the action itself; otherwise it is likely to be deferred until nightfall, when in any case a search will be made of the area over which the battalion has been fighting.
FIELD AMBULANCES.
The medical unit lying next behind a regimental aid post is one of those whose functions, though not necessarily their organization, have been considerably augmented or otherwise varied since the war began, in accordance with local requirements.
Originally its main duty was to relieve of their sick and wounded the regimental aid posts, helping them also to clear the field at nightfall or whenever there was a pause in the battle, and treating the cases until it was possible to send them to treatment centres well away from the front. It had to serve in this way simultaneously three or four battalions, all presumed to be in action on an extended front, and the better to fit it for this work a field ambulance was made divisible into three sections, each capable of acting independently, and each again divisible into a stretcher-bearer subdivision for collecting the wounded and a tent subdivision for treatment of the patients.
In several of the localities in which the British army has been fighting during the last three years field ambulances have, no doubt, been working on this plan, but in France the conditions have necessitated a modification of their work and also to some extent of their constitution.
Each remains divisible as before, and each still possesses ten vehicles for the conveyance of wounded but seven of these are now motor ambulance cars, replacing seven horse- drawn ambulance wagons, and of the nine original medical officers one has been withdrawn. Furthermore, though every A.D.M.S. (senior officer of a division) still has three field ambulances under his direct command for the work of his division, and each of these retains its capacity to work as an independent unit, he sometimes combines forces with the A.D.M.S. of another division, or the field ambulances of all the divisions of an army corps are in effect massed.
The duties they collectively perform are now practically as follows:
1. To collect the sick and wounded from battalions, whether these be actually fighting, serving as supports, or temporarily resting out of the line.
2. To decide what cases must be evacuated, and what shall be treated at the front.
3. To provide permanent treatment for those who fail to pass through the filter thus established, and for the rest temporary treatment pending evacuation.
4. To pursue a like course in respect of local sick, that is to say, cases of illness or injury arising amongst the large number of men whose presence just in the rear of the fighting line is essential to military operations.
5. To provide for the cleansing at frequent intervals of the persons of the men, the ridding of their clothes from vermin, and their disinfection when epidemic disease is in question.
6. To fill any gaps in the medical establishments of regiments, and to train medical officers and men for this work by sending them for a time to the battalions to see how regimental work is done.
7. To provide temporary assistance when needed to casualty clearing stations belonging to the army of which the divisional field ambulances form part.
8. To establish advanced operating stations for immediate emergency operations, such as those required in cases of abdominal wounds.
9. To supplement the sanitary work of battalion medical officers when the battalions concerned are located in places which are out of the fighting line but not in direct charge of the sanitary staffs of the army of which the battalions form part.
10. To do for divisions and corps any work for which provision has not yet been made by the army, and which kind of scientific knowledge medical officers commonly possess. It may be said, in short, of the British armies in France that their field ambulances are the medical bonne a tout faire of the front.
No single field ambulance ever undertakes simultaneously all the duties mentioned, and the way in which they are allocated varies; for the environment of the divisions are not identical, and the senior medical officer of each of the armies and corps on the Western front (subject to orders from a higher authority) exercises his discretion as to the fashion in which he provides for the aggregate medical requirements of the troops in his charge. The experiences of field ambulance medical officers are therefore liable to differ, more especially if the period over which they are compared is relatively short. Commonly, whatever duties have to be performed are taken in turn by each field ambulance available, the period for which it remains employed thereon varying according to circumstances.
If a division is engaged in an active part of the line its evacuation work is usually sufficient to occupy the attention of all its field ambulances, and the same is true of those of a corps when this is taking part in an advance or definite battle. In such cases the other duties are assigned to the ambulances of reserve or other divisions.
In trench warfare each division engaged generally makes its own arrangements for evacuation, the ambulances belonging to it sometimes acting as independent units, sometimes pooling their resources.
THE ADVANCED DRESSING STATION.
A section of the officers and men available is pushed up to form an advanced dressing station at some place within easy reach of the regimental aid posts of the battalions in action. They choose a place on or close to a road, so that the patients brought down from the battalion aid posts can be sent back rapidly from the advanced dressing station in wheeled vehicles to the place where the field ambulance head quarters or main dressing station has been established.
The advanced dressing station is always exposed to artillery fire, and though sometimes the crypt or cellar of a still standing but more or less wrecked building, such as a church or large schools may be available (Fig. 11)
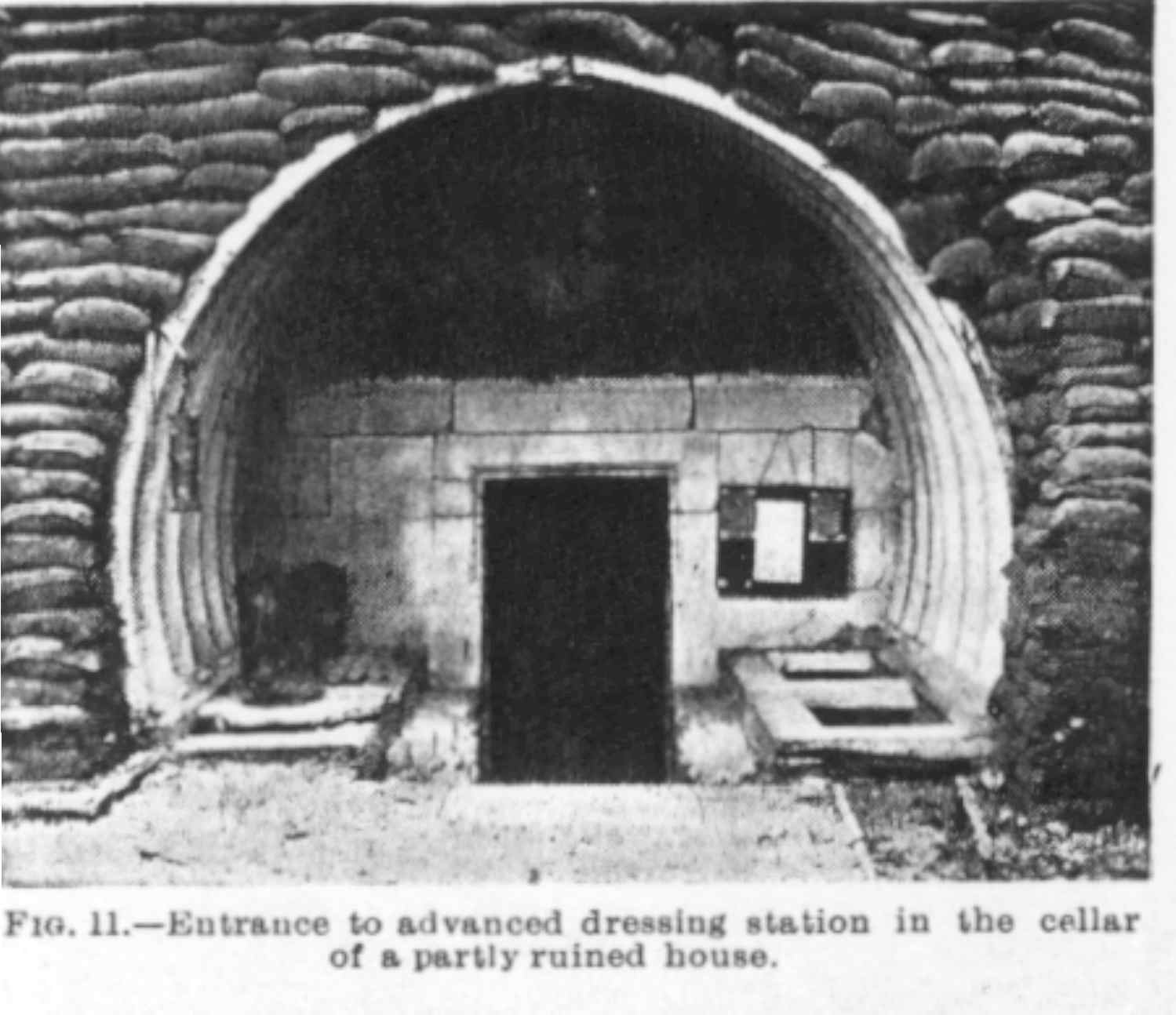
its habitation is as a rule, merely an enlarged edition of a regimental aid post. (Figs. 12 and 13.)
Fig 12
Fig. 12.- Diagram, drawn front memory of the entrance end of a small "tube" above-ground advanced dressing station. It is built of curved sheets of corrugated steel surrounded by sandbags and earth, etc.

Fig. 13.
Leading down to a dressing station 30 feet under the surface.
Its equipment and organization likewise resemble that of a regimental aid post, but is larger, because an advanced dressing station is rarely in touch with less than four regimental aid posts. To these it sends, as often as required, sufficient stretcher bearers to clear them of waiting cases, and if any considerable number of men have been left in the trenches till nightfall, it helps to remove them, and retains them till they are fit to be sent further towards the rear.
The way in which it brings down its patients varies in different parts of the line and according to the amount of fighting in progress. Sometimes patients are hand-carried all the way down through a winding communication trench a mile or more long. Sometimes they are carried straight across country, though the latter is possible only at night or when the ground traversed is dead ground-that is, an area which cannot be reached by rifle fire, and not too much hampered by wire entanglements . There are also a few places in which the trenches have an overhead tram-rail, and the wounded men can be transported on a special ambulance trolley suspended from it (Fig. 14),
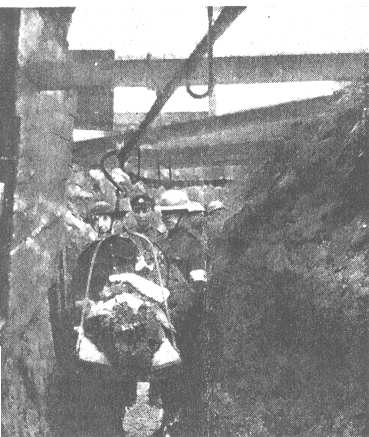
Fig. 14
The overhead trolley for bringing the wounded through the trenches.
and many areas are provided with tram-lines along which run for the greater part of the distance to be traversed small lorries capable of carrying two or four patients. There are others at which it is possible for the advanced dressing station to clear some at least of its battalion aid posts by sending up a horse ambulance. The means most commonly employed, however is a wheeled carrier, of which several types are shown in Figs. 15 and 16.

Fig. 15
A collection of wheeled stretchers and a motor ambulance

Fig. 16
A wheeled stretcher, pneumatic tyres.
Once arrived at the advanced dressing station the patients are rested, fed and dressed, if necessary, and otherwise prepared to continue their journey, which in most cases will commence as soon as ambulance cars or wagons arrive from the field ambulance headquarters or main dressing station to fetch them.

Fig. 17
Motor ambulances parked in a convoy.
ADVANCED OPERATING STATION
Commonly it is only by night that an advanced dressing station can clear the regimental aid posts with which it is in touch. In the case of an abdominal wound, however, considerations of risk from rifle and shell fire are set aside both at the regimental aid post and the advanced dressing station, and the patient is got down forthwith and sent to the rear in a special ambulance car, kept, if possible, for this purpose in a dug-out near the advanced dressing station, or summoned from the main dressing station or ambulance head quarters by telephone or messenger. The patient goes not to the main dressing station, but either straight to a casualty clearing station or to a field ambulance unit specially arranged for the instant performance of laparotomies, etc. Such a unit is called a corps or advanced operating station, and is established wherever the placing of a casualty clearing station within suitable distance of the part of the line concerned is likely to be delayed.
VARYING CONDITIONS.
The ambulance vehicles serving the advanced dressing stations almost always have to traverse roads exposed to shell fire, if not to rifle fire, and efforts are made in various ways to protect their occupants from further injury. When only trench warfare operations are in progress most of the work is done under cover of nightfall, though the depth of the darkness may be disclosed from time to time by the flashing of guns, bursting of shells, and the soaring of rockets. The ambulance transport which comes up to fetch the patients approaches and leaves the advanced dressing stations, as it were, stealthily; and, after anything like a quiet day, two or three trips at night may complete the whole evacuation.
When, however, the division or corps is taking part in an advance or definite battle the reverse is the case. Hour after hour and sometimes for weeks there is a constant inflow of stretcher-borne men, and ambulance vehicles continually arrive to carry away the patients who have received the attention they require; on these occasions the only precautions taken are to keep at a sufficient distance apart so that no single shell shall have the chance of destroying two cars, and to travel sufficiently slowly to avoid jolting the injured more than is inevitable on the shell-pitted roads. It is commonly not until the battle has commenced that an advanced dressing station can take up its position, without the site may have been chosen in advance. As it must always be on a road, so as to ensure rapid evacuation yet never run the risk of impeding the military work in progress the choice is often very limited. More likely than not it will be in a deserted trench or enemy dug-out, but it is always contrived so that the incoming and outgoing streams of wounded shall not meet, and that the more serious cases can be dressed separately from those that are slight. Provision is also made for cases which may have to be kept for some little time on account of their condition, and for protecting them from gas attacks.
Divisional Collecting Post.
The majority of cases with which it deals are "lyers" - that is to say, men who reach it on stretchers. The "Walkers" - that is to say, men who can find their own way to the rear- are usually shepherded off by patrols in advance of the dressing station to another field ambulance station known as the divisional collecting post, established when a big advance is in progress. If the area over which the corps is fighting is wide, it usually establishes two advanced dressing stations and two divisional collecting posts in different parts of the field. The field ambulance medical officers at its disposition may be sufficient for this purpose, but in respect of stretcher-bearers it is always short-handed if the fighting be really heavy, consequently on these occasions its own stretcher-bearers are reinforced from various sources. If the troops in action are very successful and make a prolonged advance, an advanced, dressing station may no sooner have established itself to its own satisfaction than it has to make a fresh move to get into close touch with the regimental aid posts.
It will be obvious from what has been said that work in and around advanced dressing stations, whether in trench warfare or in a definite battle, is attended by considerable risk. The fact that it is often exceedingly laborious may not be so apparent. If the fighting is at all heavy, the work as a whole continues without pause for many hours and while the carriage of a full-grown man over a mile or so of rough ground is never a light task, it becomes absolutely exhausting when at each stop the bearers have to drag their feet out of thick mud, and when their clothes, like those of the patient, are soaked with rain.
THE MAIN DRESSING STATION.
The main dressing station is formed by the head quarters of the field ambulance or group of field ambulances responsible for the maintenance of the advanced dressing stations. As it is liable to have to retain the sick and wounded sent down to it for some little time, it is placed sufficiently far behind the advanced dressing station to be out of range of heavy artillery fire. The exact nature of its work depends a good deal on local circumstances including the character of the fighting in progress. Sometimes it confines itself mainly to administrative work - that is to say, to classifying the cases that arrive, and distributing them for treatment according to their requirements among subsections formed by itself or other units with which it is connected; sometimes it combines this work with actual treatment. However this may be, it always arranges to rest, dry, warm, and feed the patients that reach it, and for giving them any surgical attention they need before they can safely be sent on elsewhere. It is here, too, that all cases of wounds are examined to see that antitetanus serum has been given.
The first step is necessary because, despite the greatest possible care, the transport of a wounded man from the place where he has fallen to a place as far back as a field ambulance main dressing station must always be very trying, even if his wound be not very severe, and even if his clothes are not, as is commonly the case, soaked with rain and mud. The second step is necessary because in an advance the casualties are certain to be numbered by hundreds, and while many may not need to be sent away from the real front, operations and a period of real rest may be necessary in the cases of many others before their evacuation is possible.
Cases which require evacuation are sent to a railhead hospital or casualty clearing station, and whether their detention at a main dressing station be momentary or prolonged depends - assuming transport to be available - partly on their condition and partly on the distance to be traversed to reach a railhead hospital.
For other cases it provides sometimes by furnishing treatment itself, sometimes by sending the cases on to field ambulances or other medical units set aside for the purpose of special treatment. In every corps area, for instance, if not in every divisional area, provision is made by the field ambulances for the treatment of cases of trifling sickness and injury, or of men who are temporarily exhausted or footsore. Special arrangements are also made for the treatment, without evacuation, of more or less easily cured skin diseases, such as scabies, as also for the isolation of of cases of zymotic disorder and of contact s therewith. Every army, too, has at its service centres which deal with eye cases, dental disorders, and neuroses.
The object throughout is to avoid the unnecessary evacuation of cases that can be treated at the front, for a soldier, once evacuated, is likely, how ever quick his recovery, to be lost to his unit for a considerable time, since any patient sent further to the rear than one of the treatment centres mentioned above ceases for the time being to belong to the army in which he had previously been serving, and cannot be restored to it except by passage through a regulated channel. Every patient evacuated from a field ambulance has what is known as a field medical card substituted for his regimental label. It contains particulars as to his name and army status, a diagnosis of his condition, and details as to whether he has received the requisite prophylactic doses of tetanus antitoxin, and any other information deemed likely to be useful to those who will subsequently treat him.
The accommodation provided for a field ambulance main dressing station varies according to the amount of work that it has to undertake, and may be anything from a village school to a collection of tents. Such accommodation as it possesses is arranged in much the same fashion as at an advanced dressing station, but everything is on a larger scale and the equipment more elaborate. It is thus in a position to undertake formal operations, though it usually limits itself to those essential to a patient's safe evacuation.
The heaviness of the work varies in proportion to that of the units further up the line. If the latter have been hard pressed, many of the cases will reach the field ambulance untouched except for their field dressings, and, even if nothing else be required, special splints may have to be substituted for improvised appliances. On such occasions each corps commonly provides itself with two main dressing stations lying close together, but working independently, one dealing with stretcher cases, the other with "walkers". The patients of the former reach it in ambulance wagons or cars, while those of the latter commonly arrive in char-à-bancs which have been sent up to move them as far along the road towards the scene of the fighting as these vehicles can be got. This varies, for when a big action is in progress the traffic on all available roads is very heavy, a constant stream of supplies of all kinds being essential to continued fighting.
OTHER FRONT LINE WORK.
When the work of collecting and evacuating the sick and wounded is sufficient to absorb all the personnel of the field ambulances of a division or corps, any other work which they have previously been performing is assigned to those of divisions not in action, or it is provided for in some other way. The general nature of its work is indicated in the list given of the duties commonly performed by field ambulances. When bathing establishments are run as corps or army units, and sometimes even when they are run by single divisions, the arrangements always include the provision of fresh underclothing for each man who has taken a bath. As commonly not more than ten days elapse between the bathing parades of a battalion most British soldiers change their body linen with comparative frequency, and this counts for a great deal, not only in securing their comfort, but in preserving their health.
SANITATION
The general sanitation of each army is under the super vision of an expert attached to its Director of Medical Services, while in each division there is a special sanitary section, the officer commanding it acting as sanitary expert, and advising on sanitary matters connected with the division and its component battalion and other units. Each of these sanitary sections has a small staff of non-commissioned officers and men and plenty of equipment, such as disinfecting machines, which accompany the division wherever it goes, while incinerators and the like are rapidly constructed the moment it settles down. Battalion medical officers draw their supplies of drugs, dressings, etc., from the field ambulances connected with them, and these in their turn from the advanced depots of medical stores, one or more of which is to be found in every army area.
MOTOR AMBULANCE CONVOYS.
The field ambulances are responsible for the transport of sick and wounded from the advanced dressing stations to the main dressing stations, and also, but only when working in reserve or resting troop areas, for the conveyance of sick to the casualty clearing stations. The vehicles at their disposal suffice for these purposes, though it may be necessary to supplement them. Should the fighting be heavy and the casualties numerous, these are not intended to transport patients from the main dressing stations to the casualty clearing stations. This is the work of the medical transport units, called motor ambulance convoys, one of which is allotted to every army corps (Fig. 17). It also carries to the ambulance trains the evacuable patients of any advanced hospitals which do not lie immediately alongside a railway line. They are also employed, should pressure on the work of the ambulance trains be severe, in evacuating cases from the casualty clearing stations to the base hospitals by road, and sometimes to transport individual patients whose early arrival at a base is thought advisable, and who can be got there more promptly by road than if detained for the arrival of a hospital train.
Each convoy consists of fifty vehicles, usually divided into two large, and one small section. The latter is commonly employed solely for train embarkation, and is then attached to one of the group of casualty clearing stations and works under the orders of its commanding officer and when roads are crowded by ammunition and general supply lorries, all anxious to complete their duties without loss of time, the presence of an officer with the ambulance convoy section ensures it a freer passage than it might otherwise obtain. On the other hand, there may be certain patients for whom a slow travelling pace is desirable throughout, unless the surface of the roads prove excellent - a matter about which there is always uncertainty.
Each motor ambulance car can carry six or eight patients sitting up, or four lying down. To neutralize the tendency to shock exhibited by so many wounded men the vehicles is are now generally heated automatically by the exhausts (Fig. 18), and are also provided with hot-water bottles.
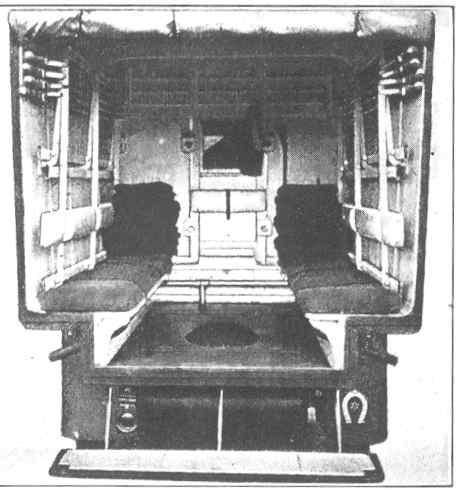
Fig 18
Interior of a motor ambulance, heated by its exhaust
The motor ambulance convoys are an outcome of the circumstances of the war in France, and an example of the ingenuity of the Royal Army Medical Corps in promptly adapting its arrangements to the needs from time to time arising. Before the war the Royal Army Medical Corps, in common with the medical services of the armies of all other countries, had to depend for the transport of casualties between advanced formations such as field ambulances, and rearward units such as railhead hospitals, on the use of supply wagons going back empty to the rear. It was the only arrangement feasible at the time, and though admittedly far from ideal, was suitable enough for the small wars in more or less uncivilized countries to which Great Britain had been accustomed, and not involving any very large number of casualties. The experience, however, of engagements at the beginning of the war showed the Director of Medical Services of the original Expeditionary Force (Sir T. Woodhouse) that the means in question would not suffice for his needs, while at the same time he found that, in the removal of patients capable of sitting up, ordinary touring cars, of which offers were made to him by various French and other residents in Paris, could be of real assistance. After some of these had been fitted with bodies very like those now used in all motor ambulance work, and others had been sent out from home, he arranged two experimental convoys, which began to work between Aisne and Paris in the first days of October 1914. experiment having proved that motor ambulances could be used with safety for long, rapid transport and over cobbled roads, and not only for short journeys in cities and suburbs, as had previously been supposed, the Director - General of Medical Services (Sir Arthur Sloggett) on his arrival in France at the end of October decided to adopt motor ambulance convoys as a definite component of the arrangement of the Royal Army Medical Corps in France. It was a decision of whose wisdom convincing evidence was quickly forthcoming.
CASUALTY CLEARING STATIONS.
The railhead hospital or casualty clearing station may theoretically be described
in several ways.
1. As the administrative junction between the lower limit of the collecting zone or front with the upper limit
of the evacuating zone or lines of communications.
2. As the focal point to which converge all roads leading from the front, and from which diverge all roads leading
to the base.
3. As the spot where road transport ends and railway or analogous transport begins.
4. As the place where all casualties collected from main dressing stations are deposited until the moment comes
for their transport through the evacuating zone to the base or distributing zone.
SELECTION OF SITE.
Two of the essentials in the selection of a site for a casualty clearing station are ready access from the front for motor convoys and free communication with the base by ambulance trains. A third is plenty of room for the necessary tents or huts, a free water supply, and safety from any but extreme range artillery fire. To find a suitable site is often difficult. Adequate room and protection from artillery fire are generally easy to secure, and water can be piped from a considerable distance, but to find a place which, besides being suitable in other respects, is readily accessible by road from the main dressing stations concerned, and lends itself to evacuation to the base by train, is much more difficult. It is a problem, in fact, which can often be solved only by running a special branch railway up to the proposed site, or by choosing a site which is on an existing railway but at a considerable distance from the main dressing stations that have to be cleared.
The first plan involves heavy expenditure of time and labour, and is usually adopted only when later on the site may be useful for some other purpose, or when the branch line can be made to serve more than one end.
The second solution is therefore the commoner, but it is to be remembered that accessibility and shortness of distance as the crow flies are not interchangeable terms. The old proverb, "The longest way round is the shortest way home," has a particular application to the transport of wounded men. Once a man is in a well-sprung pneumatic-tyred ambulance car the exact distance that he travels is of less importance than the character of the roads over which he is borne. Hence, independently of all other considerations, a site which communicates with the front by good roads is always to be preferred, even if the distance to be traversed be treble, to one which can be reached only by lanes and cart-tracks.
This is one reason why the casualty clearing stations as a whole are distributed irregularly in regard to their distance from the main dressing stations they serve. The same reason also helps to account for the differences in the habitations of casualty clearing stations. Some are in permanent buildings in towns or villages, some in huts far away from all other buildings; others in huts and tent-marquees, others in tent-marquees alone. The completely tented casualty clearing stations are usually found to be in the new parts of the line. As they settle down they acquire huts for operating theatres and administrative purposes, and if, later on, when the line moves forward, the sites that they occupy are likely to prove suitable for stationary hospitals, all the tents are replaced by huts.
THE FUNCTIONS OF A CASUALTY CLEARING STATION.
A casualty clearing station is in principle a mobile unit, since it must always keep within reasonable distance of the main dressing stations; and therefore be prepared to move when these are moved, in conformity with any change in the tactical situation of the troops they serve. Primarily it is an evacuating unit, and only intended to act as a hospital so long as it is forced by circumstances to retain its patients, and it was probably in order to keep its status well in the foreground that not long after the war began the title, "casualty clearing station" was substituted for the original term' "clearing hospital," For a corresponding reason every casualty clearing station is provided with three lorries of sufficient size to transport at a moments notice all the equipment that strictly speaking it is entitled to possess.
But however thoroughly casualty clearing stations may justify the suggestion of their title, they always go a good deal beyond it; for their functions and personnel have been adapted to existing circumstances by the D.O.M.S. in France. Hence they are no longer mere stations but real hospitals, despite the fact that some are only about six miles from the fighting line, and few lie further off than double that distance. The patients are nursed by trained women nurses; ordinary hospital beds are provided for the more serious cases; the operating theatres have usually four operating tables, are equipped with electric light, and the appliances familiar in the hospitals of large towns; and while some have x-ray annexes of their own, all have at their command the services of travelling x-ray -outfits, and clinical laboratory work is done for them by the mobile laboratories which are commonly to be found in their neighbourhood.
When a casualty clearing station has been established for some little time, the chief differences between it and a base hospital are attributable to the diversity of duties that tile casualty clearing station has to fulfil. In addition to acting as a true hospital for a short or long period, it must always be ready to operate on a very large number of patients, and to evacuate forthwith those that can safely be moved, and must also be able rapidly to prepare for immediate evacuation a very much larger number of slight cases. It must also be ready suddenly to receive and accommodate in one fashion or another an almost unlimited number of sick and wounded. Consequently, in addition to whatever accommodation in the way of actual beds it may possess, it must provide also:
1. Huts in which men lying on stretchers can be kept under cover, and receive what they require in the way of food, warmth, and surgical attention.
2. Accommodation for classifying the cases that arrive according to whether they must undergo operations under an anaesthetic, or merely require some such attention as the redressing of a wound or the replacing of a splint.
3. Accommodation for men who have received all the attentions they need, and are merely waiting to be loaded on the train.
4. Accommodation for the performance of minor surgery.
THE WORKING OF A CASUALTY CLEARING STATION.
There are considerable differences in the way different casualty clearing stations meet these needs, but in regard to definite operations the general practice is to provide sufficient accommodation and personnel for the performance of at least four operations simultaneously and continuously for an unlimited number of hours or days. Even when a battle is in progress, of the wounded men who arrive at the casualty clearing station at least 10 per cent. must visit the operating theatre before they can be sent to the base hospitals. In regard to other matters the general procedure is usually as follows: As soon as a convoy arrives the patients are all off-loaded promptly so that the ambulance shall not be detained. They are carried into a distributing room, where, while a clerk takes down particulars of his army status, etc., a medical officer decides to what class of case each patient belongs, being guided in this matter partly by his condition, partly by what is stated on his field medical card.
Thus, for instance, A, who has an abdominal wound, is sent straight to the operation-theatre preparation room. So, too, is B, who has a wound of the head and is insensible. C, who has a wound of the thigh, is sent to the stretcher case dressing-room; but D, who has an apparently corresponding wound, is for some reason in a state of profound collapse, and is therefore sent to the observation ward. E has a perforating wound of the upper thorax, and is sent to the chest ward; while F, who has a flesh wound of the shoulder, is sent to the walking case dressing-room.
When A arrives in the preparation room all his clothes are removed, and he is got ready for a laparotomy, which takes place as soon as a table in the theatre is free. B, in addition to other preparations, has his head shaved, and is sent to the theatre as soon as a surgeon and anaesthetist are ready for him. It may be decided that no craniotomy should be performed, at all events until the patient has reached a base hospital, but the case must be thoroughly examined before this conclusion is reached.
C's stretcher is placed on trestles and his wound carefully examined to see whether any operation is required; if so, he too is sent to the operating-theatre preparation room; otherwise his wound is redressed and an extension or other splint suitable for train travelling is applied.
D, on his arrival in the observation ward, is put to bed and submitted to various antishock measures until his condition is sufficiently good for an elaborate treatment of his wound.
E, on his arrival in the chest ward, is examined by a medical officer who specializes in internal medicine.
When F enters the walking-case room his bandages are taken off and the required treatment applied, unless his general condition and his field medical card clearly indicate that no further interference with the wound is likely to be desirable until he reaches a base hospital. From the dressing tent for walking cases F goes to the evacuation tent for walking cases, where he is given food and cigarettes and waits for the ambulance train; a train is usually available every day, and even oftener in times of activity; but, if there is any delay, F is given a stretcher bed and his wound is redressed in due course.
Meantime, into another evacuation tent men who belong to the various classes, A, B, C, D, E, and who have come down with the same or a previous convoy, are being brought on stretchers from the wards or other places where they have been prepared for evacuation. The standing regulation is to send on all cases to the base as soon as suitable transport is available, but any case at all likely to suffer by transport is detained as a matter of course; chest cases are never sent down until all danger of haemorrhage is presumed to have ceased, and abdominal cases are detained until they have so far recovered that they can be sent straight through to Great Britain without further treatment at the overseas base.
In any case the number of men detained is usually quite sufficient to afford the personnel plenty of ordinary hospital work between the arrival of convoys, and in order to secure time for its due performance, even when fighting is heavy in the part of the line served by the casualty clearing station and casualties are numerous, every casualty clearing station has a partner located at the same rail-head, and the two are alternately "open" and "closed" for the reception of patients. When times are quiet the commonest plan is for the casualty clearing stations concerned to open and close on alternate days. During active fighting a casualty clearing station usually declares itself "closed" when it has a given number of unevacuated patients on its hands; its partner then takes the next convoys. Should it happen that the partners are both "closed," the D.M.S. of the army concerned sends later convoys to the casualty clearing stations of some other area under his command.
Specialist Surgeons.
As a convoy does not represent a specific number of patients, and the number of convoys dispatched from any main dressing station in any twenty-four hours depends entirely upon the state of the fighting, the amount of work thrown upon a casualty clearing station varies greatly from time to time. Sometimes it resembles that of an ordinary hospital in a manufacturing town, where accidents are frequent; sometimes that of a main dressing station of so elaborate a type as to be able to perform both aseptic and septic operations, and so large as to be able to deal with 1,000 or more patients a day. Its permanent staff consists of seven medical officers, but when the fighting is heavy it is reinforced by medical officers drawn from casualty clearing stations, field ambulances, or other medical units in other parts of the line. On its permanent staff are always at least two surgeons experienced in all classes of operative work, including abdominal surgery, and the reinforcements sent when times are active include other surgeons of the same type. The net result, therefore, is that by arranging in groups the total number of surgeons and anaesthetists available, the necessary operations can be performed until the stress is over.
Distribution of Patients.
When the convoys are not large and not arriving in rapid succession, the work of distribution is done by the orderly medical officer on duty; at other times it is usual to select a surgeon of wide experience for the work, since the duty of the "spotting officer" then becomes a task of great responsibility. He must be able, for instance, to gauge rapidly the general condition of a patient and the probable degree of seriousness of his wound. In addition to bearing in mind continually how long it is likely to be before an ambulance train arrives to clear the hospital, he must keep a constant eye on the operation list. Should the latter be comparatively short or the stream of patients be falling off, his task becomes relatively easy since he can mark for the preparation room any cases which seem at all serious. In the contrary case, he must decide whether the individual and general interests would best be consulted by handing the case down to the base forthwith, Should an ambulance train be waiting or expected shortly to arrive or by keeping him, even though it is not likely to be possible to perform the operation for many hours.
Consulting Surgeons.
The clinical work of the casualty clearing stations in each army is under the supervision of an officer who in peace times is a well-known consulting surgeon, and corresponding supervision is exercised in respect of medical conditions by a physician of analogous experience.
Before being evacuated from a casualty clearing station a note is added to the field medical card of every patient as to the treatment he has received, and if an operation has been performed, or he has been treated as an ordinary hospital patient, clinical notes concerning his case for the information of the medical officers at the base are sent on in an envelope attached to a button of his bed jacket.
Many casualty clearing stations also do a certain amount of work in attending to local sick - that is to say, to cases amongst labour parties and other troops in their neighbourhood which are not in charge of a medical officer or within the area of the work of a field ambulance. It is also the rule for a casualty clearing station to detail a medical officer to afford medical attention to members of the civil population if a request to this effect is made by the local civil authority.
THE THEATRE TRAILER.
Though a casualty clearing station is a mobile unit, the transfer of so large an institution from one site to another takes a considerable time. In an advance it may be desirable to push an operating section forward at once. To meet this need the "theatre trailer" has been devised. It consists of a large pitch-pine framework, which can be clamped on to a trailer drawn by one of the lorries of the casualty clearing station. The lorry is loaded with stretchers, blankets, cooking and feeding requisites for a hundred serious surgical cases for two days, and carries also a hospital marquee and operating tent. The original idea for the trailer, as suggested by Colonel Cuthbert Wallace in September, 1916, was to fit it with shelves and pigeonholes, as on a ship. After further study, however, it was seen that it would be better to make the cupboards and other fittings movable, providing for the careful packing of their contents so that they would not suffer on the road. Each cupboard runs on four wheels, and is fitted to hold and carry without damage dressings, instruments, bowls, and enamel ware, as well as the Bowlby outfit and the marmites in use in almost every casualty clearing station theatre. There are two cupboards for sterilized dressings, overalls and towels, sufficient for one days operating, with two surgeons and four tables, dealing with 150 major operations. In addition, six complete sterilizing drums are carried, and in all sufficient dressings for 500 operations. Lotions, made up in quart bottles, are packed in a specially designed case fitted in one of the shelves. Boiled water and saline are taken in sterilized petrol tins. The instruments are packed in webbing straps stitched together and attached to the shelves. Three anaesthetic tables and folding stools are packed into two cases, which, when unpacked, can be used as surgeon's washing-up benches. The bottom shelf of each anaesthetic table contains nine compartments, each of which holds a two-pound bottle of chloroform or ether. Two other shelves contain the anaesthetic apparatus, masks, gauze, etc. Other cupboards contain primus stoves and their fuel, cleaning materials, a rack for splints, and a stand for the lotion copper cauldrons. The shelves fit one above the other, and can be built up in any order that may he desired to form dressers or small cupboards. The contents of one side lifted out of the trailer are shown in the illustration (Fig. 19).
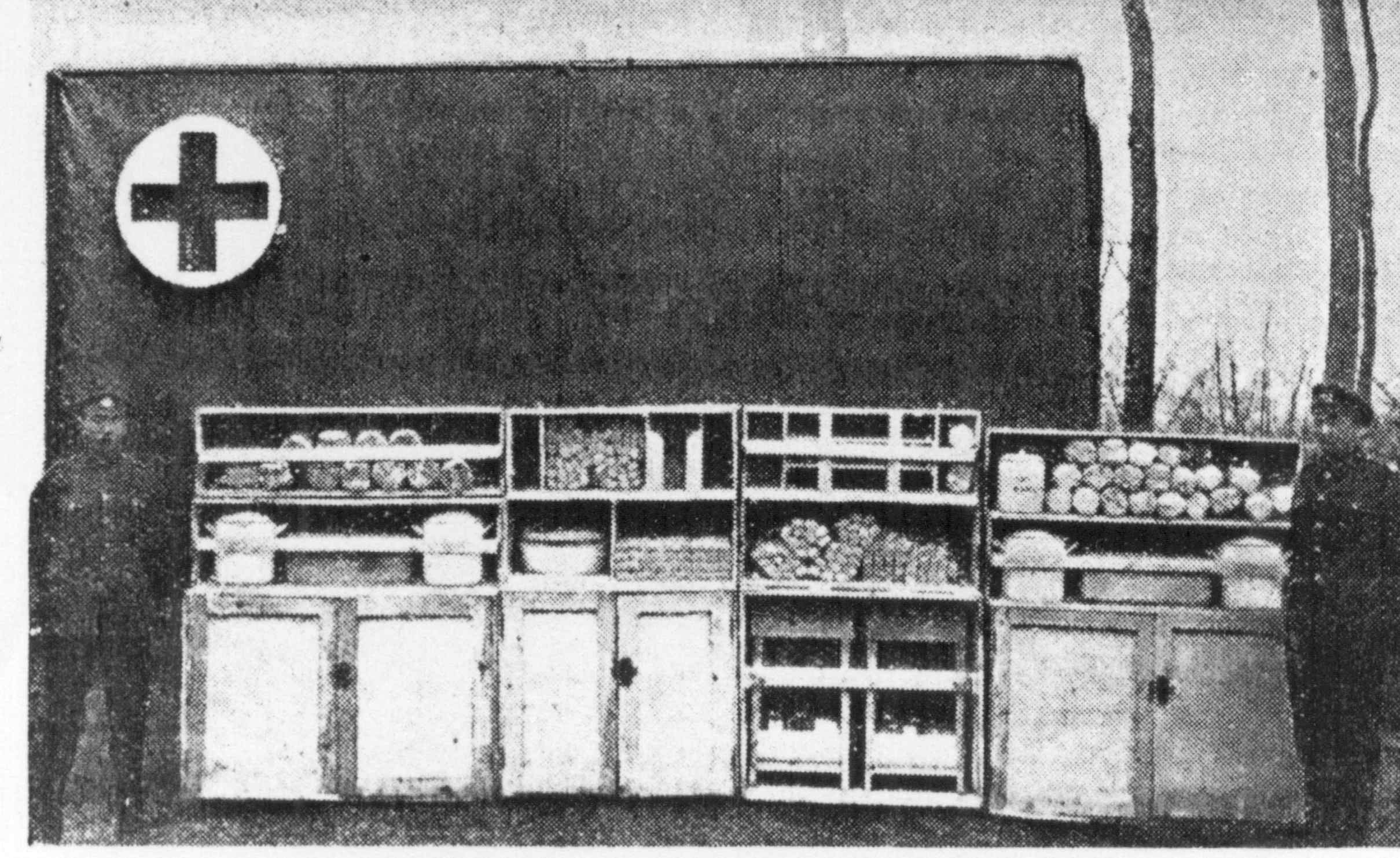
Fig. 19
Trailer with one half of its equipment unloaded. The cupboard most to the spectator's left is for dressings, the next for instruments the next contains two anaesthetic tables, and the cupboard most to the right has three compartments for splints - long splints - thigh, short splints. arm, and leg splints respectively. The shelves above the cupboards show the method of packing dressings etc.
With the trailer and trolley are four R.A.M.C. orderlies, and there are two Army Service drivers. These six men can pack the loaded furniture into the trailer in ten minutes. The main advantages of this trailer, the details of which have been worked out by Captain E. M. Cowell, R.A.M.C., and Lieutenant-Colonel G. H. Goddard, R.A.M.C., are that it ensures the careful transport of the delicate equipment of an operating theatre and provides operating room furniture ready for immediate use in all circumstances.
AMBULANCE TRAINS AND HOSPITAL BARGES.
A patient may be sent down through the evacuating zone to the base either by ambulance train, by hospital barge, or by motor convoy; in the great majority of cases the first is the method employed.
AMBULANCE TRAINS.
Several types have been used since the war began. In the early days the predominant type was made up mainly of goods vans fitted with racks to support stretchers, and supplemented by straw-strewn vans for the more lightly wounded. These trains were effective so far as actual transport was concerned, and were easy to load and unload, since the doors were wide; but the carriages could not be heated easily or kept warm, they afforded no conveniences for administrative work, and it was very difficult for the medical officers to attend to their patients once the train had started. Moreover, unless the vans were drawn from passenger trains, and this was comparatively rare, they were mounted on four wheels only, had very ineffective springs, and practically no brakes. They were gradually displaced by trains built up of ordinary passenger coaches supplemented by a saloon or restaurant car for administrative purposes. The compartments were so arranged that they could each contain four stretcher cases lying at right angles to the line of travel. Most of the coaches thus used had six wheels, and were much better sprung and braked than goods vans. They were also much better lighted, and, as a rule, each vehicle had a firebox attached exteriorly, and thus had in dependent heating. On the other band, loading and unloading was not easy, since the doors were narrow, and only rarely was it possible to arrange for intercominunication between all the carriages, so that some of them could be visited only by walking along the foot-board or by stopping the train.
A few trains of this type are still in use, but the majority belong to a third type, which is built up partly of corridor car "coaches" for patients able to sit up, partly of specially constructed "ward carriages" (Fig. 20), intercommunicating cars with tiers of berths down each side and a passage way between them.
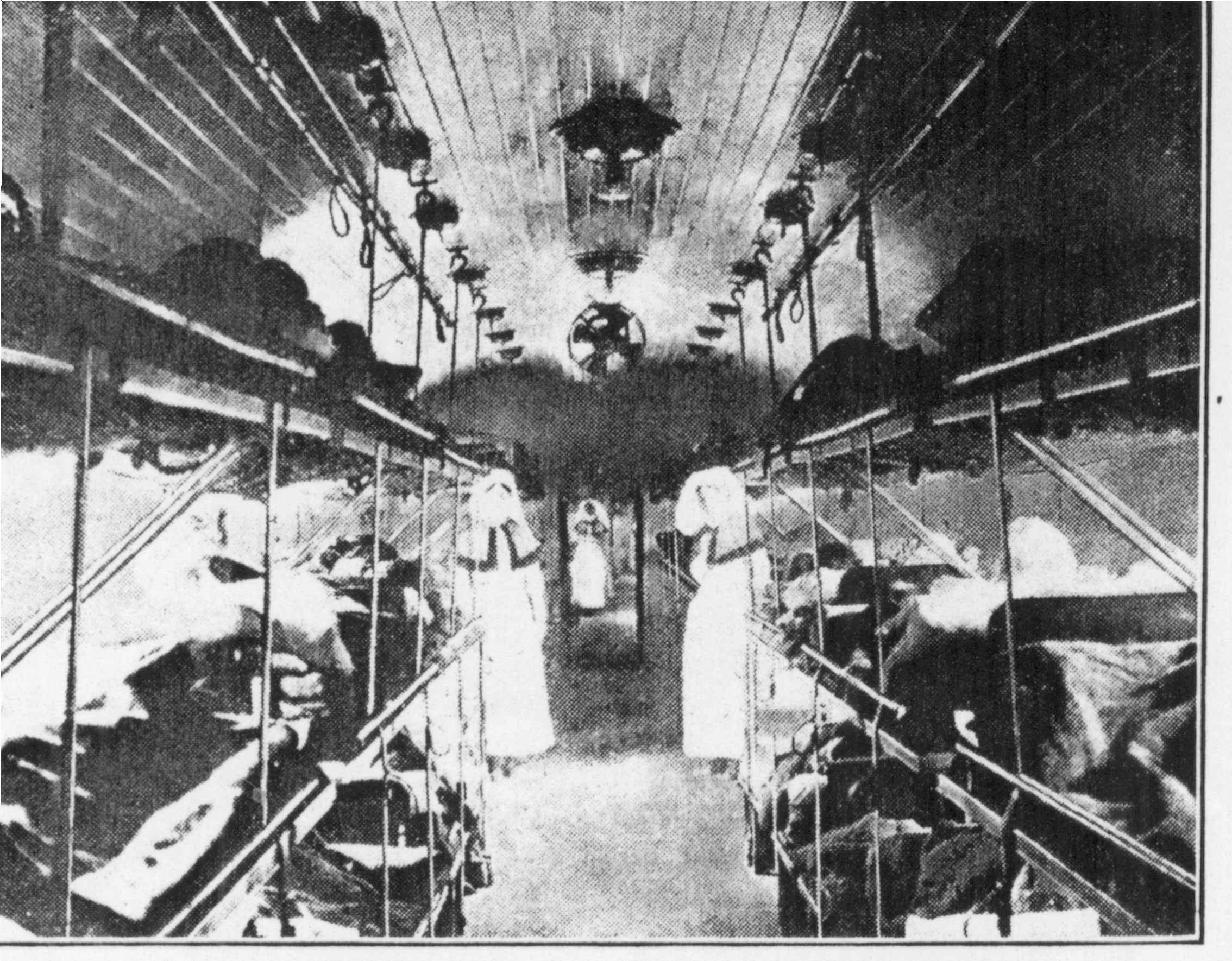
Fig. 20
Interior of a hospital train; the majority of lying cases are evacuated by ambulance train
These berths are open at the ends, and have both wire and ordinary mattresses and blankets and sheets, and the patients are habitually put to bed in them, unless for some reason, such as the existence of an injury to the spinal column, it is desired to avoid moving a patient off his stretcher. In such cases the stretcher is laid on the top of the bed. Those tiers of beds are arranged parallel to the line of travel, and as there are six sets of tiers on either side and each consists of three berths, the normal accommodation of a travelling ward is thirty-six patients, while if occasion requires, it can be increased to forty by laying stretchers in the passage way between the tiers.
The usual plan is to place the carriages in the following order, working from the engine backwards: A carriage used as an isolation ward; a coach with its compartments arranged as sleeping quarters for the medical and nursing staff; a kitchen coach; four or five ward carriages; an administrative carriage, providing an office, a room for the performance of operations (Fig. 21),

Fig 21
and a dispensary; four or five coaches for sitting-up patients; a carriage for general cooking purposes; a coach to serve as sleeping quarters for the subordinate personnel; a van for stores; and a guard's van. About 400 patients is an average load for such a train.
The "ward " carriages have wide external as well as internal doors, so that they are easy to load and unload, and the train is electrically lighted and steam heated from end to end. The wide doors of communication between the carriages afford a vista of half a dozen carriages in succession, and the actual passage may extends from one end of the train to the other. All the ward carriages, moreover, are mounted on well-sprung eight-wheeled chassis, and a Westinghouse compressed air automatic brake operates from end to end of the train. The net, result is that they are easy to work and run smoothly even over the much-used permanent ways of Northern France.
All the advantages of these trains are attained likewise in a fourth type which is the latest to come into use. In it the accommodation for patients consists entirely of ward carriages, wherein as much provision for sitting-up patients as may be required is made by turning up the middle berths of the tiers, thus leaving the upper berth for a lying-down case, while the lower one forms a sofa for three or four sitting-up patients. In the third type of train the sitting accommodation in the coaches often proves to be in excess of the requirements, so that the fourth type represents economy in engine power and rolling-stock, since, whatever the portion of lying-down cases to sitting-up cases, the whole of the accommodation can be utilized.
Ambulance trains so long as they are loaded are managed very much as if they were ordinary hospitals, but there is not usually very much dressing to do unless in a considerable proportion of the cases irrigation treatment is being applied. There are always, however, patients who require attention, and for the first hour or so, at any rate, after the train has been loaded the whole of the staff is kept busy. Once they have settled down the majority of patients sleep peacefully to the end of their journey, even those who are travelling in sitting-up coaches. They have left the battlefield behind them; they have had their wounds dressed, and all tension is at an end. This restfulness of an ambulance train, despite many physical reasons to the contrary, was noted long before the prevailing type of train came into use, and is one of the more curious psychological features of the war.
For an ambulance train of the second type the allowance of medical officers is usually three, but for the third and fourth types only two are generally required; in each case three or four sisters are carried in addition to nursing and general-duty orderlies, cooks, etc. Unless a journey is unusually long, the majority of the staff remains on duty during the time the train is loaded. As soon as the patients have been unloaded the whole train has to be cleaned, bed-linen changed, dirty linen dispatched to the wash, and fresh supplies of stores obtained, so that rest for an ambulance staff does not come until the up-country journey has commenced.
The movements of the trains as a whole are regulated by a medical officer of the staff of the D.M.S. Lines of communication. If a full load is not waiting at any wingle rail-head, several are visited in succession. Once loaded the train travels at a rate of about 12 miles an hour to its destination at the base which may be anything from fifty to a hundred miles away. Information as to the hour of its probable arrival is telegraphed to an officer at its destination, who meets the train with a sufficient number of stretcher-bearers and motor ambulance cars to distribute the patients promptly among the various hospitals at this base.
HOSPITAL BARGES
Evacuation by hospital barges is necessarily restricted to parts of the front traversed by navigable canals, and also by the fact that comparatively few casualty clearing stations lie sufficiently near canals; for patients to be embarked without an intermediate journey in an ambulance car. This means of evacuation is slow, but is of use in dealing with patients for where it is desired to secure absolute freedom from shaking. Barges, however, are not used solely for evacuating purposes; in certain parts of the line they can be taken close up to main dressing stations and advanced operating stations, and can then be used either to provide additional accommodation or practically as if they were travelling casualty clearing stations, chest and abdominal cases being placed straight on board after operation and taken down to a port, where they are evacuated to a home base by being loaded on a hospital ship.
The barges used are those familiar on Flemish canals (Fig. 22).

Fig. 22
Hospital barge being towed
When one end of the interior has been partitioned off into cabins for the staff, and the other into a kitchen, scullery, and quarters for the subordinate personnel, there remains ample room in the middle for thirty ordinary hospital beds arranged fifteen on each side with a passage between them. There is a space amidships into which patients are lowered from the dock above by means of a hand lift. This space can be used for the performance of operations if necessary. Except that its ceiling is low (about 10 ft.) and its diameter comparatively narrow (about 16 ft.), a barge ward looks very much like a hospital ward (Fig. 23).
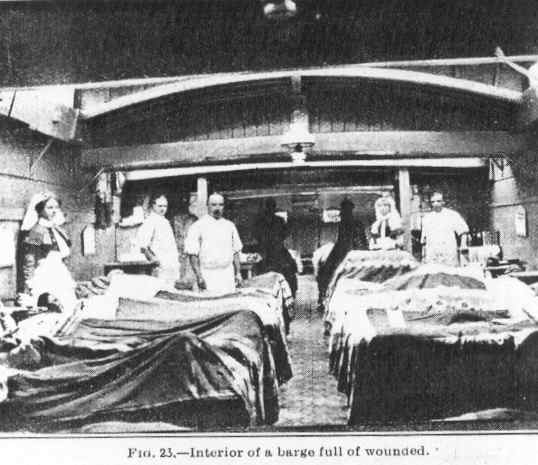
Fig. 23
All the barges are provided with a dynamo and gas engine; they can be lighted either by electricity or by removing one or more sections of the deck which forms the ceiling of the ward. They are drawn by a tug in charge of men accustomed to canal work. They are divided into flotillas of four, but more often than not they travel singly or in couples. Every barge carries two trained women nurses in addition to nursing orderlies, general orderlies, and cooks. Each barge also carries a medical officer, unless two barges or more are travelling together, and then one is sufficient for all of them. The average duration of a barge journey is from twenty-four to forty-eight hours. They travel only by daylight, and at the rate of about three miles an hour.
STATIONARY HOSPITALS.
At places along the railways traversing the evacuating zone there are medical units known as stationary hospitals. These in theory are 200-bed hospitals of comparatively simple equipment as compared with that of a general hospital. Their bedsteads, for instance, are folding iron "barrack bed-steads," and they are not supposed to have clinical laboratories or x-ray annexes. In France, however, nearly all stationary hospitals are capable of accommodating several times their regulation number of patients, and many in point of equipment and extent of accommodation do not differ from the large general hospitals in the distributing zone, unless they are used to fulfil some special aim.
Such of these units as are in the evacuating zone do their work in direct association with main dressing stations, and since the dispatch of a patient to them does not necessarily entail his formal evacuation, they are almost to be regarded as annexes thereto and therefore as front-line units. The rest are used for the reception and treatment of cases of sickness and injury among troops on the lines of communication and for cases which the medical officers in charge of ambulance trains may think it desirable to off-load at the earliest possible moment. Strictly speaking, a stationary hospital is not entitled to more than seven medical officers but it is allotted a larger number if it accommodates more than its regulation number of patients, and is doing work which for its due performance requires an augmentation of the staff.
CONTROL.
It is from general head quarters that the Director-General of Medical Services usually controls the whole of the medical work of the front through the Directors of Medical Services of the different armies, as also that of the evacuating zone and the distributing zone through the Director of Medical Services Lines of Communication.
The operations thus controlled include not only the distribution and maintenance of hospitals and other medical units, together with all the arrangements for the evacuation of patients from the front to the bases and from the bases to the United Kingdom, but also certain other important branches of work. These are the distribution of medical reinforcements, the co-ordination of action throughout the whole British force in regard to sanitation and the prevention of epidemic disease, and the work of weeding out from the armies men who, though still useful soldiers, are not capable of doing front-line work, many of whom must eventually be sent home to be discharged from the army.
At the same place are also held the periodic meetings of a council formed by the Director-General of Medical Services to assist him in the settlement of questions from time to time arising. It consists of eight members and is so constituted that the temporary and permanent elements of the medical service of the army, general and bacteriological hygiene, medical and surgical work at the front, the same work at the bases, and administration throughout the whole area, are all represented in equal proportions.
There is a second council of the same general kind, which includes the whole of the civilian consultant specialists holding temporary commissions in the army, as well as the principal permanent officers on the staff of the Director-General of Medical Services. But this meets less often owing to the difficulty of withdrawing so many officers from their ordinary work simultaneously.
THE DISTRIBUTING ZONE.
The hospitals to which the patients are sent on their arrival in the distributing zone are known as general and stationary hospitals. The former are in theory much larger and more comprehensively equipped than the latter. In practice, however, there is in France often no difference even in point of size, and invariably both afford the same facilities for the best forms of medical and surgical work. That is to say, their ward equipment is of the same kind as in large civil hospitals in times of peace, they have all large and annexes, and bacteriological laboratories and x-ray annexes.
ORGANIZATION OF GENERAL AND STATIONARY HOSPITALS.
In point of size every stationary hospital can now accommodate at least 500 patients instead of the regulation 200, and every general hospital at least 1,040 instead of 520. The larger figures represent the number of beds kept at all times ready for the reception of patients. In time of pressure the accommodation can be increased by some 50 per cent. The clinical work is divided into a medical and a surgical division, each in charge of a specialist assisted by ward medical officers. To the surgical division there are also attached specialists in operative surgery who vary in number according to the accommodation of the hospital.
The nursing is done by trained women, those appointed to each ward working under the supervision of a ward sister, who is subject in her turn to the hospital matron. There are also a certain number of orderlies trained in nursing duties, who assist and on occasion replace the women nurses, and of general duty orderlies who do all the rough work of the hospital. The male personnel is under the control of a non-commissioned officer commonly called a wardmaster, who is subject in his turn to the sergeant-major of the hospital. Supplies of every kind are obtained by the quartermaster, who is responsible for their due preparation. He holds honorary rank as an officer in the Royal Army Medical Corps, and to attain this position he must not only possess tact and good manners but must pass examinations in general education and technical and military subjects spread over so many years that most quartermasters are men who have entered the corps at a very early age.
The laboratory and x-ray rooms are in the charge of specialists, privates or noncommissioned officers who have received training in these duties being appointed to assist them. The institution as a whole does its work under the control of an officer of the rank of lieutenant-colonel or colonel, who in the larger hospitals has a registrar to assist him in the keeping of medical records. In times of pressure this officer commonly takes charge of a certain number of beds, and often also acts as company officer or adjutant, his work including disciplinary control of the more military side of the work of the unit.
A few hospitals occupy large buildings, such as casinos or hotels, but most of them now lie in camps outside the towns, of which they nominally form part. They are formed sometimes of huts alone, sometimes of huts and marquees. The marquees have boarded floors, stoves, and electric lighting and double roofs. In fine weather the whole of one side of a marquee can be removed, the patients being thus kept practically in the open air; the officer in the Royal Army Medical Corps, and to attain this position he must not only possess tact and good manners but must pass examinations in general education and technical and military subjects spread over so many years that most quartermasters are men who have entered the corps at a very early age.
But, although base hospitals are well equipped and managed on identical principles, they are differentiated to
some extent by the character of their work. At each base, for instance, one hospital deals solely with infectious
diseases, while the rest, though prepared to take cases of all kinds, habitually specialize in the treatment of
some particular class of injury or disease - for example, skin disorders, ophthalmic troubles, jaw injuries, nerve
complaints, head cases, and fracture, of the lower extremities. There are also some base hospitals which, owing
to their distance from evacuation points, deal mainly with comparatively light cases.
At all base hospitals the time for which serious cases may be retained is not limited, but the general rule is to transfer to Great Britain any cases which are deemed fit for transport and are not likely to be fit for active service again in less than three weeks. Patients who complete their treatment in the base hospitals are sent on their discharge to convalescent depots, where they remain for a varying number of days, and thereafter, if considered fit once more for the front, are sent to the depots of the regiment or corps to which they belong. In the contrary case they are marked as base details and are kept under medical observation in barracks and employed on duties of various kinds
BASE MEDICAL STORE DEPOTS.
Other medical establishments at the base are depots of base medical stores (Fig. 24),
Fig. 24
A store for an ambulance train
whence all the up-country depots, as well as the local hospitals and ambulance trains, draw their supplies, and the base hygiene laboratories, whose main work is to test the purity of the food supplies of the troops. There is also at one base a large bacteriological laboratory devoted solely to research work, and much work of the same kind also goes on at the laboratories attached to the different hospitals. Sometimes the work is done as an independent effort, sometimes in co-operation with the officers in charge of the mobile laboratories in the collecting zone, and as a means of testing how far the results there obtained are supported by observations made on patients who have reached a later stage of their illness or injury.
LABORATORIES: MEDICAL HISTORY.
The general control of all the laboratories and of their work in the investigation of the problems of epidemic disease is the special charge of an Adviser in Pathology to the Director-General of Medical Services. In addition two officers appointed by the Director-General represent the Medical Research Committee of Great Britain; their duty is to advise upon the systematic recording of clinical notes, so that the requisite data may be available for general medical statistics and for pension claims, and also to secure that the various new types of disease and injury seen in this war are made the subject of specific study from a clinical and a pathological point of view by selected officers. As comparatively few cases remain in the hospitals in France throughout their whole course, the work involves securing continuance of study of many of the cases on their arrival at home. The aim in view is to secure that all the data necessary for the formation hereafter of sound opinions as to the medical lessons of this war shall be duly forthcoming.
As in the various army areas, the clinical work at each base is supervised by consulting specialists in various branches of medicine and surgery, and dissemination of newly acquired knowledge is secured partly by memorandums issued from time to time by the Director-General of Medical Services, partly by meetings of medical societies established not only at the bases but in the collecting zone, and partly by publication of results in the medical press.
The base hospitals are also used as depots for medical reinforcements, officers newly arrived from home being appointed to them, both in order that they may gain some experience of general routine, and also to enable the authorities to ascertain their physical and other aptitudes for work of various orders. The younger men are sent eventually to field ambulances and thence to regiments.
OVERSEAS CONTINGENTS.
All the great British dominions beyond the seas - India Australia, New Zealand, Canada, and South Africa - have medical units in the field, though they are all worked on the same system as units which are strictly speaking Royal Army Medical Corps units, and they are all under the control of the Director-General of Medical Services.
There have been one or two hospitals officered entirely by volunteers supplied by the faculties of certain universities in the United States of America, and some units working under the aegis of the British Red Cross Society. These also have been under the general control of the Director. General of the British Medical Service.
GENERAL ADMINISTRATION
In most of the military Hospitals in France the administrative work is done by permanent officers of the Royal Army Medical Corps, and the bulk of the executive work by temporary officers, who contract to serve for the year, but in most cases renew their contracts as a matter of course. For the first eighteen months or more all these officers were volunteers, but since all men under 41 are now liable for military service, a considerable proportion of those now arriving are selected by civilian Medical War Committees, in response to the demands of the War Office. In making the selection the committees have regard not only to the fitness of the individual for foreign service, but also to the question of his indispensability or otherwise from the point of view of the civil population among which he has been practising.
Intermediate between these two orders come a certain number of officers who have received commissions for the duration of the war, and who are usually doing special work of some kind, and a large number of Territorial and Special Reserve officers. The former are civilian medical practitioners who long before the war joined the volunteer body known as the Territorial Army as medical officers, and by taking part in annual exercises and in other ways acquired a general knowledge of military routine. The Territorial army was mobilized with the Regular army on the outbreak of war, and these Territorial officers, belonging as they did to regiments and field ambulances, were at first to be found almost exclusively in the front line formations, but many of them now hold administrative positions and posts as divisional medical officers of hospitals. The Special Reserve officers are usually young men who before the war undertook to serve in the Royal Army Medical Corps if required, and meantime went through a course of three-months training, receiving a small retaining fee in respect of each year their names were kept on the roll.
The nursing staff is drawn from an equally large number of sources. Some belong to the Regular army, others to the hospitals which in peace nominally form part of the Territorial army, others are nurses who in peace work independently, and many come from the overseas commonwealths.
The great variety in the components of the R.A.M.C. is a source of strength, since it ensures the inclusion of men of varied talents and representative of special knowledge of all branches of medicine and surgery. The whole corps is administered in a spirit which secures unity of effort among men of different mental constitution and previous experience, yet without trammeling individuality by the imposition of other than necessary rules and regulations. It is to this that is mainly to be attributed the successful working of the Royal Army Medical Corps in France, but material assistance has also been derived from the sympathy extended towards all medical affairs for the benefit of the troops by the Commander-in-Chief.
SEA TRANSPORT.
The motor convoys at the front are army units, but the ambulance cars by which patients are taken from the base hospitals for shipment to England are maintained by the British Red Cross Society, and at some bases are driven by women. As not all the bases are at a port, a short journey in an ambulance train sometimes intervenes between a patient's departure from a base hospital and his embarkation.
The embarkation medical officer is informed day by day as to how many patients are waiting shipment, and the proportion of lying to walking cases, and as soon as a ship is ready notifies each hospital concerned how many patients of each kind he can accommodate. Arrived at the quay-side, the ambulances are unloaded under the supervision of the embarkation medical officer, and as each case reaches the dock it is assigned a position on board according to its nature. Swing cots are used for the severer cases, since they can be approached from both sides, and to the less severe are assigned berths arranged in tiers. On long voyages walking cases are also given berths, but on short ones they are allowed to sit or stroll about as they please as soon as each man has been clad in a life-jacket. The next step generally is the serving of a meal and the distribution of cigarettes.
Meantime the lying-down cases are being treated as if they were still in a hospital on land, for every hospital ship has a staff of surgeons and nurses and all the equipment necessary for hospital work. All hospital ships have previously been passenger vessels, and the necessary room for wards is provided partly by re-equipping the dining and other saloons for their new use, partly by clearing the lower decks of cabins. Lifts are provided for moving patients, and the vessels are painted white, with a green band painted from stem to stern with a red cross painted in the middle. At night there is a long row of red and green lights along the taffrail on both sides.
HOME HOSPITALS.
Arrived at the port of destination the patients are received by a disembarkation medical officer and his staff, who have been warned by wireless telegraphy of the number of patients on board, and have caused to be brought up to the quay-side the requisite number of hospital trains; these trains are then loaded rapidly by stretcher-bearer parties and dispatched to different parts of Great Britain. The more serious cases are usually sent to hospitals in the neighbourhood of London or the great provincial towns. Some of the larger institutions are military hospitals which existed before the war, but the great majority have been specially created. Some of these, however, previously had a nominal existence as Territorial hospitals, it being part of the system of the Territorial Force that at each local centre the larger civil hospitals should undertake to open if required a military hospital officered by medical men selected from their own staffs. The officers thus selected were given commissions à la suite in the medical department of the Territorial Force. Apart from large military hospitals of this and other kinds, including some maintained by the British and other Red Cross societies, a considerable proportion of all civil hospitals now have arrangements for the reception of military patients who are treated by the civilian staffs attached to those hospitals.
All the larger hospitals have special departments for patients whose successful treatment involves knowledge of one or other of the special branches of medicine and surgery. There are also very numerous convalescent homes, and the orthopaedic hospitals described by Dr. Colin Mackenzie (BRITISH MEDICAL JOURNAL, May 26th, 1917, p. 669 et seq.). Finally, there are numbers of camps to which are sent men who it is expected will recover their fitness for active service when they have undergone remediable exercises of various kinds and a general physical training.
The duty of seeing that an adequate number of hospitals for military patients are maintained in Great Britain, as also that of providing the reinforcements and stores required for the medical work of the armies in France, the Balkans, Mesopotamia, India, East Africa and elsewhere appertains to the Director General of Army Medical Services in London, a post filled since November 1914, by Surgeon-General Sir Alfred Keogh. He had held the same office some years previously and had returned to it in order to allow the actual occupant of the post, Sir Arthur Sloggett, to take up work which it was realised would be of weekly increasing importance and for which his talents and experience seemed, and have abundantly since proved, specially to fit him - namely, the control of the medical affairs of the British armies in France. It is on the arrangements of these armies that this description of the work of the Royal Army Medical Corps is based.
So far as the British people are concerned the work of the Royal Army Medical Corps has given the greatest satisfaction, and it is believed that after the war, when details become known to those capable of assessing its more scientific aspects, it will be acknowledged that the corps has taken full advantage of opportunity offered for advancing its precise knowledge of medicine and surgery as well as of means of advancing vast numbers of sick and wounded men.